Current Size: 100%
You are here
Home » About Glaucoma » Types of GlaucomaNarrow Angle Glaucoma
Narrow or Closed Angle Glaucoma
Introduction
In the anterior or front part of the eye, aqueous fluid is produced and travels to the drainage structures of the Trabecular meshwork as shown in Fig 1.
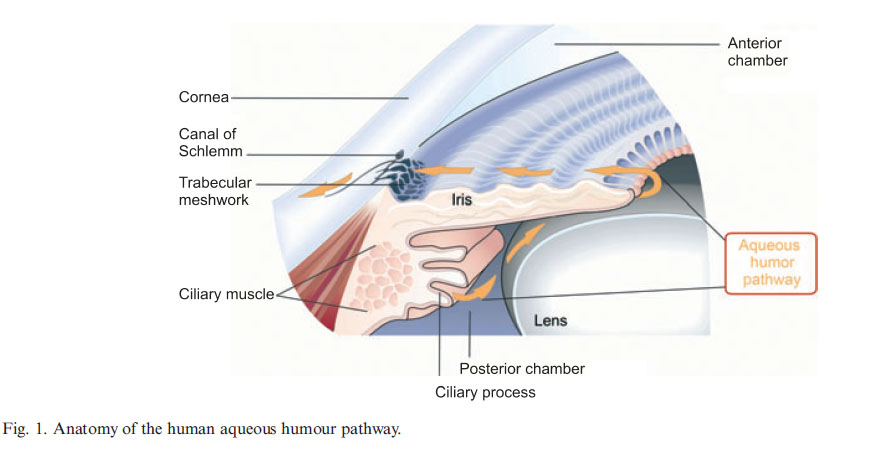 Notice that as the fluid moves around the lens and through the pupil, it passes in front of the iris to its final destination, the Trabecular meshwork (drain). There is an angle formed by the front part of the iris at its edge near the Trabecular and the cornea (commonly referred to as the iridocorneal angle). In the case of a narrow or closed angle, this angle becomes reduced so that the final path to the drain is obstructed. There can be different grades or degrees by which this angle becomes narrowed - and slightly different physiological causes. In the case of complete angle closure, the fluid can no longer reach the drain resulting in large increases of intraocular pressure.
Notice that as the fluid moves around the lens and through the pupil, it passes in front of the iris to its final destination, the Trabecular meshwork (drain). There is an angle formed by the front part of the iris at its edge near the Trabecular and the cornea (commonly referred to as the iridocorneal angle). In the case of a narrow or closed angle, this angle becomes reduced so that the final path to the drain is obstructed. There can be different grades or degrees by which this angle becomes narrowed - and slightly different physiological causes. In the case of complete angle closure, the fluid can no longer reach the drain resulting in large increases of intraocular pressure.
Causes of Narrow angle glaucoma - Many factors can result in the iris being pushed or pulled forward resulting in a decrease of the angle as noted above. There may be periodic episodes of angle closure or there may be a full closure resulting in a medical emergency.
- Farsightedness or hyperopia: People with these eyes may have a shorter axial length resulting in crowding of the front eye structures
- Pupillary Block: As seen in Figure 1, the ciliary body produces aqueous fluid and in some cases it is trapped due to the adhering of the iris to the lens (blocking the passage around the lens). This results in pressure which pushes the iris forward and a narrowing angle increasing IOP.
- Plateau Iris: This is an anatomical configuration where the ciliary process is too close to the iris causing a plateau instead of a concave in the iris. This can result in the iris tissue bunching up around the drain and causing blockage. Dilation of the pupil via light restriction or miotic therapy can cause the iris to further cover the drain causing a possible angle closure attack or IOP spike.
Risks
- Gender: Among Caucasians, narrow or closed angle glaucoma occurs approximately 3 times more often in females as in males.
- Race: Peoples which have narrower anterior chambers have a higher incidence of narrow angle glaucoma or CAG (closed angle glaucoma). Typically, this includes Asians, Intuits, and people of northern European descent.
- Age: As we get older, the lens becomes thicker and can crowd the anterior structures, decreasing the angle, and increasing the risk of pupillary block.
Diagnosis and symptoms
Someone with a narrowing angle or angle closure may not have any symptoms unless there is considerable increase in eye pressure. The symptoms may include foggy vision, seeing halos around lights, pain and redness in and around the eye. Most symptoms when they occur, may constitute a medical emergency and therefore, receiving immediate medical attention is of utmost importance. There can be partial, intermittent closure so that pressure spikes may occur with or without symptoms. Many with narrow angles do not have ocular hypertension or POAG, so pressure spikes may not be evident on routine screening. However, CAG and POAG may be overlapping conditions and appear simultaneously in certain individuals.
The diagnosis of narrow (or closed) angles is usually done via an examination of the front structures of the eye using a gonioscope. This may be done with or without dilation drops - a doctor may not dilate if concerned about inducing an angle closure or pupillary block with the enlargement of the pupil. The doctor will closely examine the amount of space formed by the angle and see how visible the resulting drainage structures appear. The doctor will also note any scarring around the drain and also observe the configuration of the iris to determine whether there is any plateau feature. Scarring might occur with repeated rubbing of the iris against the drainage structures. Though complete occlusion or closing of the angle resulting in an emergency situation is not common, when it does occur, it can threaten vision.
Treatment for narrow angles or CAG
Traditional pressure lowering drops used for POAG may be of little use in CAG because of the different mechanism involved in elevated eye pressures (the drain is blocked in CAG as opposed to the TM not functioning properly in POAG). At one time, medications like pilocarpine were used for CAG because they reduced the size of the pupil and thus helped pull the iris away from the drainage structures. However, because of side effects and the possibility of pupillary block in a small percentage of patients, they are no longer commonly used for this purpose. The standard treatment currently is an 'Iridotomy' whereby a laser is used to create a small hole in the iris (essentially creating another pupil. This extra route allows aqueous fluid to move freely to the front part of the iris and thereby relieves pressure behind the iris (which can otherwise bow forward reducing the angle and blocking the drain).
For 3d animations illustrating the above principles, please watch narrow angle glaucoma and also laser iridotomy treatment for narrow angles.

Login or Create an Account to start interacting with the FitEyes community.